56 years old male presented to the Gm op
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan. is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
56 YEARS OLD MALE PRESENTED WITH
Chief complaints:
Weakness in both left upper limb and lower limb since 2 years
Pain in the Right hip and ankle joint since 4 days
History of presenting illness :
patient was apparently asymptomatic 2years ago then he developed weakness in the left upper limb and lower limb - sudden in onset started after finishing his work and returning home at 6:00 pm . immediately went to local hospital and CT was done and started on medication.Took medication for 6months and then stopped taking medication weakness gradually increase to difficulty in walking
N/H/O loss of sensation, N/H/O loss of consciousness, N/H/O up rolling of eye balls, involuntary movements of UL and LL drooling of saliva or deviation of angle of mouth ,uses of homeopathic medication for 1year and stopped.
Pain in the Right hip and ankle joint since 4days
N/H/O trauma / fall
Past history:
N/k/c/o HTN /DM/CAO/THYROID/SEIZURES DISORDER
Personal history:
Diet - mixed
Appetite -Normal
Bowel and bladder - regular
Sleep - adequate
Addiction - Nill
Treatment history :
Not significant
Family history: Not significant
General examination:
Patient was conscious,coherent, cooperative ,moderately built and Nourished
Vitals :
BP-110/70mmhg
PR -82bpm
RR -18cpm
Temp-96.8F
SPO2-95% at RA
GRBS -124
No pedal edema ,lymphadenopathy ,pallor,icterus,clubbing
Systemic examination:
CNS EXAMINATION: GCS -E4 V5 M6
Gait - circumduction gait
HIGHER MENTAL FUNCTIONS:
Conscious, oriented to time place and person.
Speech : Normal
Behavior : is not aggitated and not irritable
Memory : Normal
Intelligence : Normal
CRANIAL NERVE EXAMINATION:
1st : Normal
2nd : visual acuity is normal
3rd,4th,6th : Normal
5th : sensory intact
7th : Ability to blow cheeks
8th : No abnormality noted.
9th,10th : palatal movements present and equal.
11th,12th : normal.
MOTOR EXAMINATION: Right Left
RT LT
POWER - UL 5/5. 3/5
LL 5/5. . 3/5
TONE. - U L N Hyper
LL N. Hyper
REFLEXS - biceps. 1+. 3+
Triceps 1+. 3+
Supinator. - 2+
Knee 1+. 3+
Ankle. 1+. 2+
Plantar flexed
SENSORY EXAMINATION:
SPINOTHALAMIC SENSATION:
Crude touch - normal
pain felt on upper limb
Supraorbital pressure felt
Sternalrub pain felt
DORSAL COLUMN SENSATION:
Fine touch able to perceive on right upper and lower limb
CEREBELLAR EXAMINATION:
Finger nose test able to perform with both hand
Nystagmus not seen
SIGNS OF MENINGEAL IRRITATION: absent
GAIT: circumduction gait
Respiratory system:
Inspection: chest shape normal,
No scars , no engorged veins
Movement of chest both sides
AUSCULTATION :
Bilateral air entry
Normal vesicular breath sounds
PALPATION:
Trachea central
Cvs :
Inspection:
There are no chest wall abnormalities
The position of the trachea is central.
Apical impulse is not observed.
There are no other visible pulsations, dilated and engorged veins, surgical scars or sinuses.
Palpation:
Apex beat was localised in the 5th intercostal space 2cm lateral to the mid clavicular line
Position of trachea was central
There we no parasternal heave , thrills, tender points.
Auscultation:
S1 and S2 were heard
There were no added sounds / murmurs.
Abdominal examination:
Shape : scaphoid
Tenderness -no
Free fluid -no
Liver,spleen -not palpable





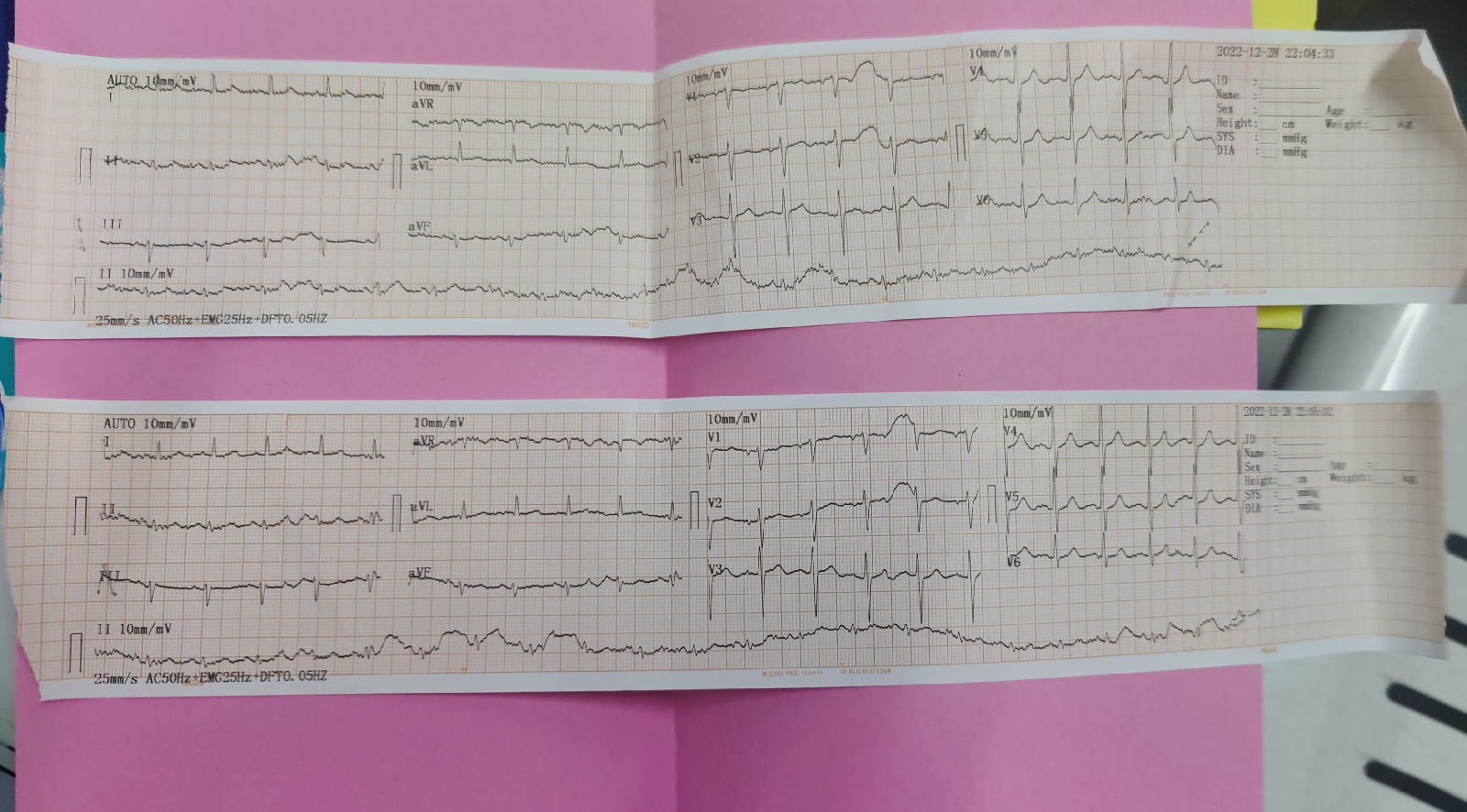
Investigation:
Diagnosis : known case of CVA with HEMIPLEGIA


Comments
Post a Comment