50Years old female
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan. is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
50YEARS OLD FEMALE PATIENT CAME TO GM OPD WITH
CHIEF COMPLIANTS:
Abdominal pain since 5months
Itchy lesions on abdomen since 1 year
HOPI :
Patient was apparently asymptomatic 5 months ago then she developed abdominal pain insidious in onset non progressive in epigastric region and right hypochondrium,later progressive to diffuse abdominal pain. pain is more after eating food,not radiating.
N/H/O vomiting,loose stools ,hematemesis,fever ,cough ,SOB, palpitations.
occasionally pedal edema present .
Itchy lesion on abdomen since 1 year (took treatment)
PAST HISTORY:
N/H/O similar complaints in the past
N/K/C/O DM ,HTN ,TB ,ASTHMA , THYROID, EPILEPSY.
PERSONAL HISTORY:
Appetite: Normal
Sleep - Adequate
Bowel and bladder - Regular
Addiction - occasional toddy intake
TREATMENT HISTORY:
Not significant
FAMILY HISTORY:
Not significant
GENERAL EXAMINATION:
Patient is concious, coherent, cooperative
Well built and Nourished.
Vitals :
BP -140/90
PR-78
RR-18
TEMP -96.8
No pallor, icterus, clubbing, cynosis
Pedal edema - occasionally present (Non pitting type )
SYSTEMIC EXAMINATION:
RESPIRATORY SYSTEM:
Inspection: chest shape normal,
No scars , no engorged veins
Movement of chest both sides
AUSCULTATION :
Bilateral air entry
Normal vesicular breath sounds
PALPATION:
Trachea central
CVS :
S1,S2 - heard
No murmur
Abdominal examination:
Shape : scaphoid
Tenderness -no
Free fluid -no
Liver,spleen -not palpable
CNS:
Higher mental status intact
REFLEXES are intact
No focal neurological deficit




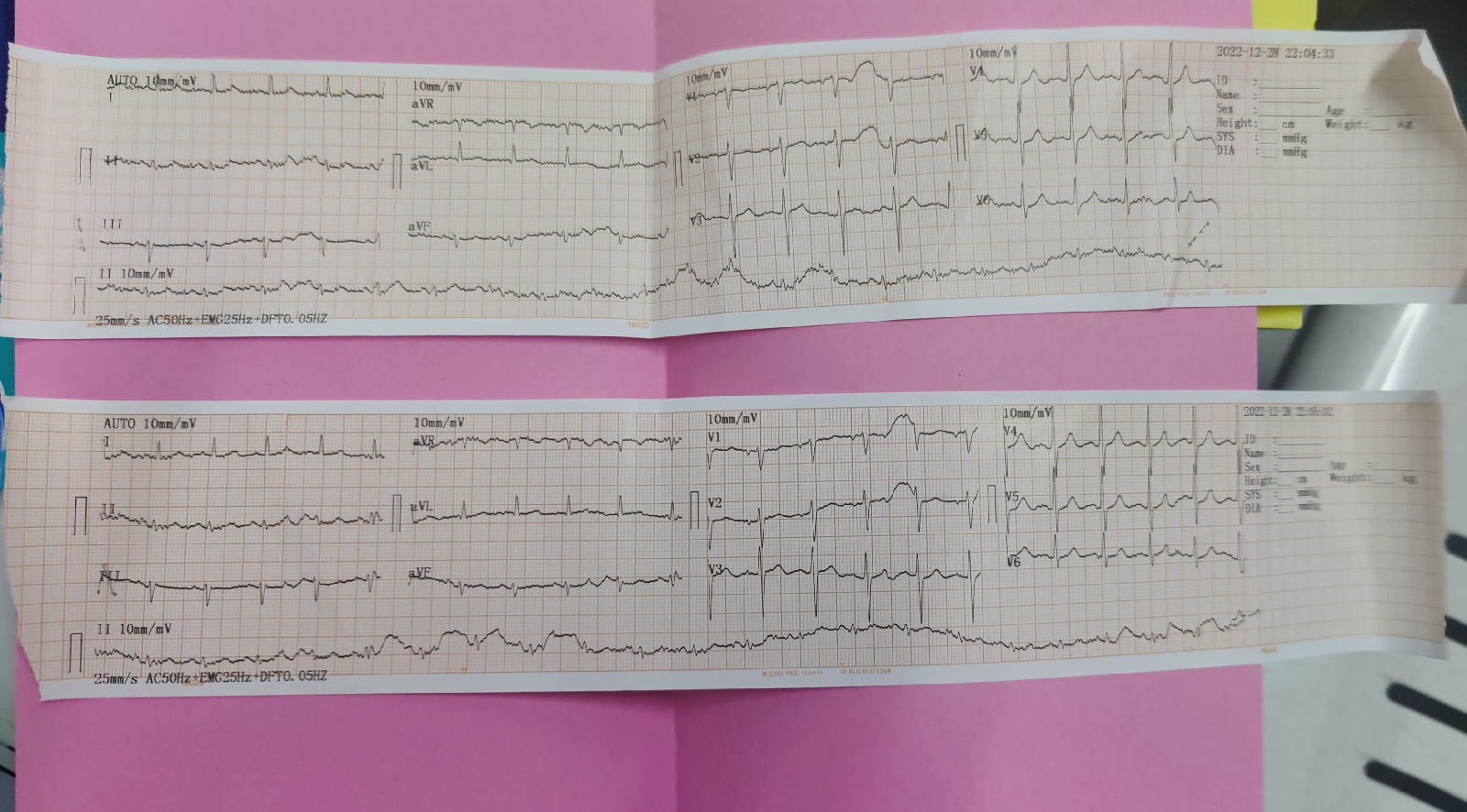
ECG :

Other :

USG :
IMPRESSION- GARADE 2 FATTY LIVER
DIAGNOSIS:
? ALCOHOL GASTRITIS ? FATTY LIVER


Comments
Post a Comment